Selner's Rhinolaryngoscopy Online

John C. Selner, MD
William K. Dolen, MD
Bryan Spofford, MD
Jerald W. Koepke, MD
Endoscopic Images and Annotations - 4. The Larynx
Endoscopic Images and Annotations - 1. The Nasal Cavity
Endoscopic Images and Annotations - 2. The Nasopharynx
Endoscopic Images and Annotations - 3. The Oropharynx
Larynx
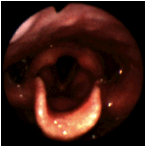 |
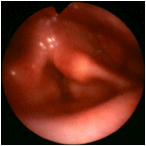
The posterior wall of the hypopharynx is at the top of the slide with the U-shaped epiglottis at the bottom. The aryepiglottic folds and the arytenoids are located immediately behind the epiglottis. Deeper in the larynx, one can see the pink false cords and the lighter true cords which are framed by the epiglottis. To the right and to the left of the larynx are the piriform sinuses, gutter like structures which direct food around the larynx and into the esophagus. Only the upper 1/3 to 1/2 of the piriform sinuses are ordinarily visualized in a laryngeal examination. (Selner slide #18) |
 |
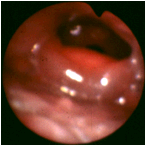
An orientation similar to the previous image, but a closer view taken with a right angle telescope in order to provide more details. Anterior to the epiglottis, at 4 and 8 o'clock are the 2 cup-shaped valleculae. At 6 o ' clock is the median glossoepiglottic fold. At 3 o' clock and 9 o ' clock are the lateral glossoepiglottic folds. The valleculae represent the most posterior extension to the base of the tongue. In the center of the slide is the aperture of the glottis, a triangular structure defined by the true vocal cords and the posterior commissure between the arytenoids. The true cords are whitish since they are less vascular than the false vocal cords located superior and lateral to them. In this slide, they are the pinker structures lateral to the true vocal cords. Between the true vocal cords and the false vocal cords are the laryngeal ventricles. The nodular swellings located in the aryepiglottic folds are the corniculate cartilages which actually sit on top of the true arytenoid bone structure. (Selner slide #19) |
 |
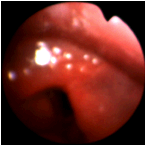
In this closer view of a normal larynx, the true and false vocal cords are more clearly identified. |
 |
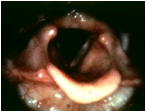
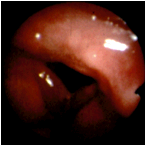
The larynx is seen in phonation with the corniculate cartilages in the aryepiglottic folds, partially obstructing the view of the true cords. There is some asymmetry of this larynx in phonation, but it is within normal limits. The upper portion of the piriform sinuses is well visualized. They are open and symmetric. (Selner slide #20) |
 |
A 45 year old gentleman attributed his progressive voice muffling to allergic disease. Between the arytenoids in the posterior commissure is a smooth marble-sized mass compromising the glottis. The pathology report identified this laryngeal mass as a benign schwannoma, an extremely rare laryngeal tumor. |
 |
This 65 year old lady had well-documented allergic rhinitis and had been successfully treated with allergen immunotherapy. She and her physician attributed her progressive hoarseness to allergy. At surgery, these lesions were benign papillomas, although malignancy was in the differential diagnosis in this smoker. |
 |
More papillomas of the vocal cords. |
 |
Arytenoid edema. |
 |
Laryngeal edema. |
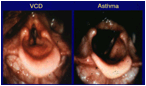 |
In patients with vocal cord dysfunction syndrome, the vocal cords adduct, forming a posterior diamond-shaped opening as seen on the left figure. This finding is not present in asthma (right figure). |
 |
Another example of vocal cord dysfunction syndrome. |
 |
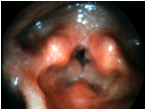
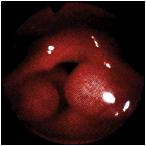
A patient with asthma and symptoms of gastroesophageal reflux. The whole supraglottic larynx is bright red, consistent with an acid burn. Although red, the epiglottis does not appear to be thickened. Reflux can cause inflammation of almost any part of the upper aerodigestive tract, including the nose. (Selner slide #48) |
 |
A closer view of the larynx of the patient with reflux, in the previous image. (Selner slide #49) |
 |
This is the larynx of the same patient in the previous 2 images after maximal medical management for gastroesophageal reflux. The erythematous reaction of the glottic tissues has subsided. However, chronic inflammation has resulted in irregularity of the true cords. (Selner slide #50) |
 |
A patient with chronic asthma requiring chronic inhaled steroid medications noted vague throat complaints. The posterior hypopharyngeal wall is located at 12 o'clock, and the anterior commissure of the larynx is at 6 o'clock. The arrow is pointing to a papillomatous lesion on the posterior hypopharyngeal wall. The papilloma was subsequently removed under general anesthesia and proved to be a squamous papilloma, which was an incidental finding not related to corticosteroid therapy. (Selner slide #51) |
 |
This 58 year old patient presented with bizarre neuromuscular weakness and complaints of glottic irritation upon exposure to solder fumes. The anterior commissure of the larynx is located at 6 o'clock. The pink tissue originating from the patient' s left false vocal cord is a residual papilloma resulting from juvenile papillomatosis. (Selner slide #52) |
 |
Right true vocal cord paralysis post thyroidectomy. The right cord is paramedian; the immobility would be much more clearly visualized in a dynamic situation. The asymmetric glottis is open. (Selner slide #53) |
 |
The same patient as in the previous image, attempting to adduct the cords. In this pair of slides, note that the asymmetry is most apparent by observing the position change of the left arytenoid. The left cord crosses the midline with phonation in order to close the larynx when protecting the lower airway from aspiration. (Selner slide #54) |
 |
A patient with vocal cord paralysis that did not spontaneously migrate to the midline position. Surgical displacement of the cord was accomplished by injection of Teflon paste deep to the muscle many years ago. The left true vocal cord demonstrates a foreign body granuloma which has formed presumably due to migration of the Teflon into the submucosa. (Selner slide #55) |
 |
This patient presented with a history of mild swelling of the left maxillary area and a minimal sensation of swelling of the tongue. She had experienced a mild sensation of "irregularity" in her throat, but had no dysphonia or dysphagia. The pointer is on the posterior pharyngeal wall and the base of the tongue is at 6 o'clock. The red, edematous structure in the center of the slide is the epiglottis. This angioedema of a critical part of the airway is potentially life threatening. (Selner slide #56) |
 |
This is a 40 year old, with known walnut sensitivity, who unknowingly ingested walnuts in the form of a finely ground powder added to blueberry muffins for a flavoring enhancement. The pointer is on the posterior hypopharyngeal wall. The glottis is at 6 o'clock. The edematous dumbbell structures crossing the midportion of the slide are markedly edematous mucosa overlying the arytenoids. (Selner slide #57) |
 |
Some 30 years prior to this examination, this patient developed hoarseness and a masculine voice character coincident with clinical polio. It had been thought that weakness of the vocal cords coincident with the polio was responsible for the voice quality change. The patient is a smoker. The glottis is located in the center of the slide. The anterior commissure is at 6 o'clock. The true vocal cords are not readily recognized because of the fusiform edema affecting the membranous vocal cords. This is a classic Reinke's edema which was being inappropriately attributed to the patient' s past history of polio. The edema is thought to be the result of chronic irritation of the vocal cords associated with cigarette smoking. Vocal cord stripping and laser photocoagulation in conjunction with cessation of smoking resulted in normalization of voice quality. (Selner slide #58) |
 |
A nodule is present on the anterior third of the right true vocal cord, with a smaller nodule on the left cord. Vocal nodules are usually paired and located at the midportions of the membranous cords. Since the posterior third of the vocal cord is the vocal process of the arytenoid, the midportion of the membranous cord appears to be at the junction between the posterior two-thirds and anterior on-third of thecord. The tracheal rings and the cricothyroid cartilage are seen in the distance, distal to the glottic aperture. (Selner slide #59) |
 |
This gentleman had a long history of asthma with seasonal worsening in conjunction with classic pollinosis symptoms. He had noted increasing exercise induced shortness of breath. The pointer is on the posterior pharyngeal wall. A tiny glottic aperture can be visualized in the center of the slide. Two huge cystic structures originating in the right and left false cords are encroaching on the glottic airway. Following surgical correction of these laryngoceles, he has residual mild asthma and has had almost total relief from the exercise related symptoms. (Selner slide #60) |
In memoriam, John Canty Selner, MD (1936-2006)