
Endoscopic Images and Annotations - 1. The Nasal Cavity
Endoscopic Images and Annotations - 2. The Nasopharynx
Endoscopic Images and Annotations - 4. The Larynx
 |
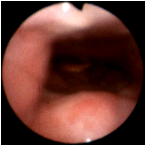
The oropharynx in a normal individual. The uvula at 5 o'clock is resting on the posterior tongue. The epiglottis can be seen above and slightly to the left in this view. |
 |
Prominent lingual tonsils. |
 |
Even larger lingual tonsils. |
 |
This is a 37 year old female who underwent adenoidectomy and palatine tonsillectomy at the age of 3 years. As an adult, she complained of a globus sensation and of having something which she could not swallow chronically stuck in her throat. Her symptoms were dismissed as neurotic. There is massive hypertrophy of the remaining lingual tonsils. The posterior oropharyngeal wall is at 12 o'clock, and the base of the tongue is at 6 o'clock. (Selner slide #45) |
 |
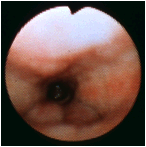
In this view, the endoscope is passed through the choana and is directed caudally from the left posterior nasal passage. At 12 o'clock is the posterior pharyngeal wall, and immediately posterior to this tissue are the vertebral bodies. The prominent ridge at 6 o'clock is the muscularis uvulae as seen from above. In the distance, one can see the tip of the epiglottis. Distances tend to be exaggerated by the wide viewing angle of the endoscope. (Selner slide #16) |
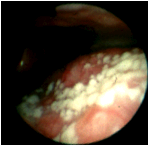 |
The base of the tongue is at the bottom of this image, and the posterior pharyngeal wall is at the top. The examiner can ask the patient to lean forward and protrude his tongue in order to obtain a clear view of the hypopharynx . This posterior tongue demonstrates the circumvallate papillae, which are the prominent pink nodules, and the whitish structures, which is keratin on the filiform papillae. Sometimes the white filiform papillae can be confused with Candida infection. (Selner slide #17) |
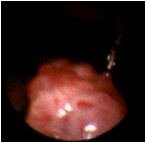 |
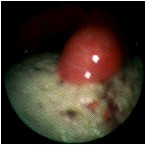
Uvular granuloma, a potential premalignant lesion, which was not discernible on routine physical examination employing a tongue depressor. (Selner slide #40) |
 |
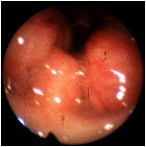
A patient with long standing chronic rhinosinusitis. The tip of the examining scope is in the nasopharynx, and is directed inferiorly. At 12 o'clock is the posterior pharyngeal wall. The tip of the epiglottis is seen in the distance in the center of the slide. Prominent lymphoid nodularity can be readily visualized on the posterior wall . The palatine tonsils protrude from the lateral walls at 4 o'clock and 9 o'clock. (Selner slide #41) |
 |
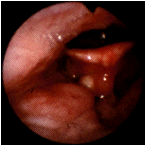
Significant enlargement of the palatine tonsils at 2 o'clock and 7 o'clock producing airway obstruction. The uvula is visible between the palatine tonsils. (Selner slide #42) |
 |
A child with a clinical history suggesting obstructive sleep apnea. The narrow airway caliber as seen in this view represents significant obstruction from hypertrophy or hyperplasia of the palatine tonsils. (Selner slide #43) |
 |
Pharyngeal spasm in a patient complaining of tightness of the throat due to exposure to copy machine chemicals and carbonless copy paper. The diameter of the oropharynx has been remarkably reduced by spasm of the pharyngeal constrictor muscles. At the base of the slide, the lingual tonsils are compressed. The epiglottis is barely visible, distal to the obstruction. (Selner slide #44) |
 |
During the course of a viral illness, a 27 year old male began to experience a focal painful sensation in the back of the tongue. On the base of the tongue, there is an erythematous nodular lesion which appeared to be an inflamed, edematous circumvallate papilla. The lesion resolved spontaneously. (Selner slide #46) |
 |
A 3 mm mucocele is visualized in the floor of the left vallecula; the lingual tonsil is located at 7 o'clock. Mucoceles are commonly located about the faucial arches and the epiglottis. This lesion did not require further investigation or treatment. Sometimes, though, a mucocele will become large enough to produce symptoms because of its size. Occasionally, a mucocele can become infected (mucopyocele). (Selner slide # 47) |
In memoriam, John Canty Selner, MD (1936-2006)