Endoscopic Images and Annotations - 2. The Nasopharynx
Endoscopic Images and Annotations - 3. The Oropharynx
Endoscopic Images and Annotations - 4. The Larynx
 |
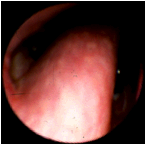
This is a view of a normal right anterior nasal cavity. The septum is on the right. The inferior turbinate and the inferior meatus are on the left. |
 |
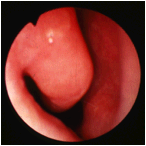
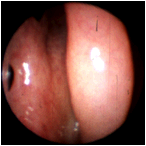
A nasal septal deviation caused by dislocation of the quadrangular cartilage off the maxillary crest and onto the floor of the nasal passage. The anterior end of the inferior turbinate is on the left. The mucosa is slightly more erythematous than normal. This inflammation may be due to turbulence in the nose caused by distortion of the architecture. (Selner slide #24) |
 |
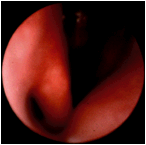
A relatively small but patent right nasoantral window, opening into the lateral wall of the inferior meatus. The right inferior turbinate is identified by the pointer. The floor of the nose is at 6 o'clock. (Selner slide #21) |
 |
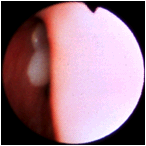
By inserting the rhinoscope through a patent antral window, one may assess the condition of the sinus mucosa. Compared to the nasal mucosa, normal sinus mucosa is whiter and less vascular. (Selner slide #22) |
 |
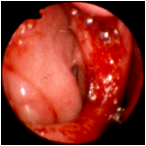
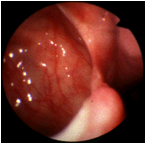
This is a view of a normal floor of the right posterior nasal passage. The prominent vessels are normal. The whitish structure at 10 o'clock is a light reflex off the posterior end of the inferior turbinate. Behind this structure is an incomplete view of the medial margin of the torus tubarius, surrounding the eustachian tube orifice. The oval opening of the choana is partially visualized. The structure at the back of this view is the adenoidal pad, which may be inflamed. The adenoid is usually more pale than the surrounding structures. |
 |
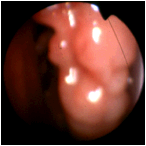
This patient complained of nosebleeds, crusting and a whistling sound when breathing through the nose. This view from the anterior end of the left nasal passage demonstrates a large septal perforation secondary to trauma and subsequent infection of a septal hematoma. Fortunately, the patient did not develop a saddle nose deformity. The patient's right nasal passage may be visualized through the perforation from the left side. The right superior and middle turbinates are visible through the perforation. (Selner slide #26) |
 |
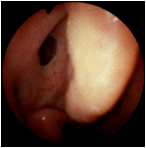
A ridge of septal cartilage which has created a groove in the left inferior turbinate. This condition may be associated with referred pain in the maxillary area resembling that of sinusitis. In the upper left quadrant is the inferior portion of the inferior turbinate. At 6 o'clock is the floor of the nose. (Selner slide #25) |
 |
In this view of the superior portion of the mid nasal passage, a septal spur is seen impinging on the medial surface of the middle turbinate. At some point in the past, this patient had received a direct blow to the nose, causing the posterior portion of the septal (quadrangular) cartilage to displace from its articulation with the bony structures of the septum. This results in facial pain when the patient develops nasal congestion - a symptom complex sometimes called Sluder syndrome. |
 |
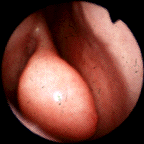
This polyp originates from the inferior surface of the inferior turbinate, and rests on the floor of the nose at 6 o'clock; the inferior turbinate is at 11 o'clock. The polyp's origin can be identified by palpation with a cotton-tipped applicator. This kind of polyp is not readily movable, and it is easily distinguished from the majority of polyps which originate via the middle meatus from the anterior ethmoid cells. (Selner slide #29) |
 |
A view of the anterior left nasal passage with the endoscope directed superiorly. The middle turbinate is seen with the neck of the turbinate attaching to the roof of the nose. The septum is located to the left in this slide and the middle meatus is on the right. The middle turbinate is prominent; a CT might show a concha bullosa. (Selner slide #9) |
 |
The right nasal passage and middle meatus with the middle turbinate extending from 12 o'clock to 6 o'clock. The septum is to the right of the middle turbinate, and the middle meatus is to the left. In the middle meatus the cleft is the hiatus semilunaris. Superior and to the right of the hiatus, and resembling a second middle turbinate, is the bulla ethmoidalis. (Selner slide #10) |
 |
Polypoid degeneration of the posterior inferior turbinate in the left nasal passage, often referred to as a mulberry turbinate. (Selner slide #31) |
 |
Polypoid degeneration of the middle turbinate in the right nasal passage. (Selner slide 30) |
 |
The right middle meatus is visualized with the endoscope tip directed superiorly. The mucosal surface on the right is the inferior aspect of the middle turbinate. A sinus ostium is located at 9 o'clock. This structure could be a maxillary sinus ostium or the ostium of an anterior ethmoid sinus. The ostium is located slightly anterior to the semilunar hiatus with the ethmoid bulb partially visualized behind it. (Selner slide #11) |
 |
An accessory ostium of the right maxillary sinus. Visualization of the sinus mucosa is possible when the size of the ostium permits. |
 |
A large antral window created in the middle meatus of a patient with chronic sinusitis. |
 |
A closer view showing the mucosa of the maxillary sinus. |
 |
An even closer view. |
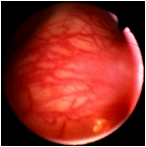 |
Vascular engorgement of the maxillary sinus mucosa is present following challenge with cigarette smoke. (Selner slide #23) |
 |
The left middle meatus is occupied by a single ethmoid polyp which is displacing the middle turbinate toward the septum located at 9 o'clock. Characteristic features of a polyp, distinguishing it from nasal mucosa, include the slightly yellow or translucent coloring of a smooth relatively avascular structure. This polyp can be moved with a cotton-tipped applicator, indicating its origin from the middle meatus. (Selner slide #27) |
 |
The right sphenoethmoidal recess in a normal individual. The septum is medial. Lateral at the 6 o'clock position is the ostium of the sphenoid sinus. The superior turbinate crosses from 1 o'clock to 7 o'clock. The lateral structure at 11 o'clock is the ostium of a posterior ethmoid sinus. |
|
|
14. The rhinoscope is on the floor of the left nasal passage, with its tip directed superiorly to visualize the sphenoethmoidal recess. The septum is at 9 o'clock. The superior turbinate is in the center of the slide. The sphenoid sinus ostium is at 9 o'clock and a posterior ethmoid ostium is at 2 o'clock in the superior meatus. (Selner slide #14) |
 |
The right posterior superior nasal passage, looking into the sphenoethmoidal recess. The nasal septum is on the right. Mucopurulent drainage is emanating from the sphenoid sinus. Similar purulent drainage was also noted from the ethmoid ostia. This is an indication of sinus inflammation, but presence or absence of exudate can not be relied on to establish the presence of infection. (Selner slide #33) |
In memoriam, John Canty Selner, MD (1936-2006)